
Glaucoma is one of the leading causes of irreversible blindness worldwide and remains a significant public health challenge in India. A major concern is that structural damage to the optic nerve begins years before patients notice symptoms. By the time visual field defects appear, nearly 30–50 percent of retinal ganglion cells may already be lost. Optical Coherence Tomography (OCT) has revolutionized early glaucoma detection by identifying structural biomarkers long before functional loss becomes evident. Understanding these OCT biomarkers is essential for clinicians aiming at early diagnosis, timely intervention, and prevention of blindness.
In countries like India, late presentation, lack of awareness, and limited screening programs contribute to higher glaucoma-related blindness compared to the Western world. Since glaucoma damage is irreversible, the only effective strategy to prevent blindness is early diagnosis, proper risk stratification, timely treatment, and regular monitoring. OCT plays a critical role in achieving these goals by detecting microscopic structural changes before visual symptoms develop.
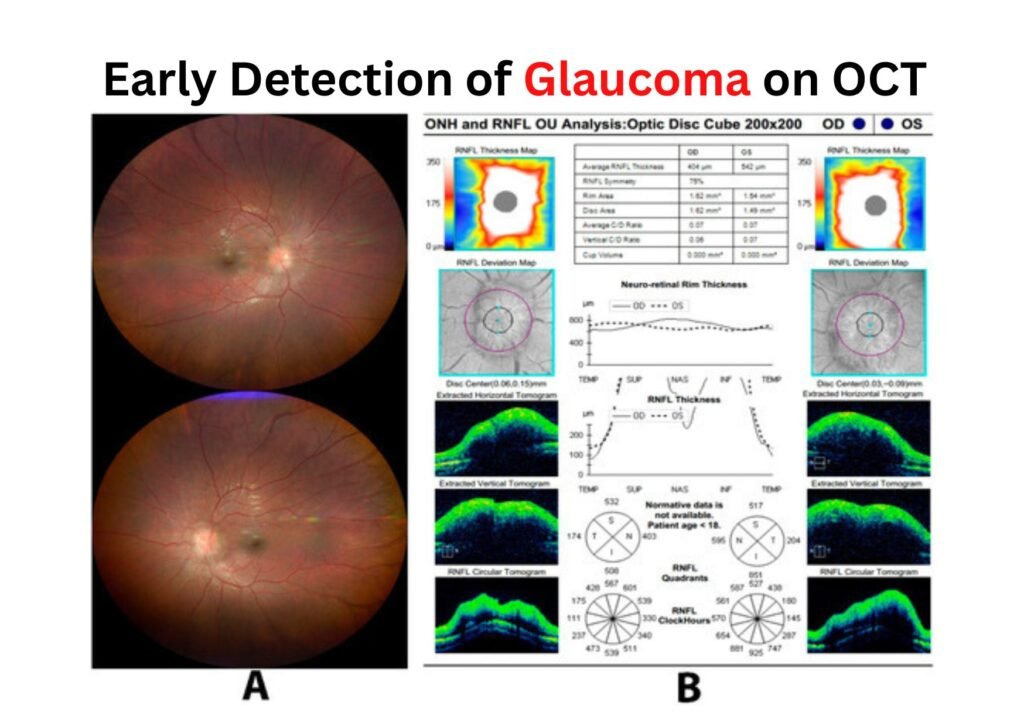
Among the most important OCT biomarkers for early glaucoma detection is peripapillary retinal nerve fiber layer (pRNFL) thickness. This parameter measures the thickness of nerve fibers around the optic disc. In early glaucoma, focal thinning—often beginning in the inferior or superior quadrants—may be observed. Asymmetry between both eyes and deviation from the normative database are early warning signs. RNFL thinning frequently precedes visual field defects, and even a loss of 5–10 microns may indicate early disease. Inferior RNFL thinning is the most common early structural change seen in glaucoma.
Another highly sensitive biomarker is the ganglion cell complex (GCC) or ganglion cell-inner plexiform layer (GCIPL), which evaluates the macular ganglion cell layer and inner plexiform layer. Early glaucoma changes include localized macular thinning, particularly in the inferotemporal region, along with early asymmetry. Since nearly 50 percent of retinal ganglion cells are located in the macula, GCC analysis is extremely valuable for early detection. In some patients, especially those with pre-perimetric glaucoma, GCC thinning may appear even before RNFL thinning.
Bruch’s membrane opening–minimum rim width (BMO-MRW) is another advanced structural biomarker. It measures the shortest distance from Bruch’s membrane opening to the internal limiting membrane, providing an anatomically accurate assessment of the neuroretinal rim. Early glaucoma changes include reduced rim width and sectoral thinning. Compared to traditional disc margin-based assessments, BMO-MRW offers better reproducibility and improved early detection accuracy.
Optic nerve head parameters also contribute to early diagnosis. Indicators such as increased cup-to-disc ratio, reduced rim area, increased cup volume, and vertical elongation of the cup may be observed. However, optic nerve head parameters alone are generally less sensitive than RNFL or GCC analysis in very early disease, though they become valuable when interpreted alongside other biomarkers.
Macular thickness and asymmetry analysis further enhance early detection. Evaluating inter-eye and intra-eye macular thickness differences can reveal subtle superior-inferior asymmetry or focal macular thinning. Macular asymmetry analysis is emerging as a particularly sensitive early biomarker, especially in cases of normal-tension glaucoma.
OCT angiography (OCTA) adds a vascular dimension to glaucoma evaluation. It measures peripapillary and macular vessel density. Early glaucomatous changes may include reduced peripapillary capillary density, microvascular dropout, and focal perfusion defects. In some cases, especially normal-tension glaucoma, OCTA may detect microvascular compromise even before significant RNFL thinning becomes apparent.
A crucial stage in glaucoma management is pre-perimetric glaucoma, where structural damage is visible on OCT but visual field defects have not yet developed. At this stage, biomarkers such as GCC thinning, focal RNFL defects, BMO-MRW reduction, and macular asymmetry are particularly useful. Detecting glaucoma during this critical window can prevent future functional vision loss.
Monitoring progression is equally important as early detection. Progressive RNFL thinning beyond normal age-related loss, increasing focal loss volume in GCC analysis, trend-based thinning analysis, and event-based progression alerts are key indicators of disease advancement. Combining structural OCT findings with visual field progression enhances diagnostic confidence and improves patient management.
Understanding the structure–function relationship is vital. In early glaucoma, structural loss typically precedes functional loss. In moderate to advanced stages, however, visual fields may continue to worsen even when RNFL thinning plateaus due to the floor effect. Therefore, OCT is especially valuable in glaucoma suspects, patients with ocular hypertension, early disease, and individuals with a strong family history.
Artificial intelligence is shaping the future of glaucoma diagnostics. AI-assisted OCT analysis can detect subtle patterns that may be missed by clinicians, improve reproducibility, identify high-risk individuals, and predict progression. Deep learning models integrating RNFL, GCC, and vascular parameters are showing promising results in enhancing early diagnosis accuracy.
From a practical clinical perspective, every glaucoma suspect should undergo comprehensive OCT evaluation including pRNFL measurement, GCC or GCIPL analysis, BMO-MRW assessment, asymmetry evaluation, and comparison with normative databases. Clinical correlation with intraocular pressure, optic disc examination, and pachymetry remains essential. Repeat scans are important to confirm suspicious findings, as a single abnormal scan does not confirm glaucoma. Consistency and reproducibility are key.
From a public health standpoint, the burden of undiagnosed glaucoma in India remains high. Incorporating OCT into screening programs for high-risk groups, especially individuals above 40 years of age with a family history of glaucoma, can significantly reduce blindness. Hospitals, tertiary eye centers, and charitable eye institutions can play a transformative role by integrating OCT-based early detection protocols into outreach and community programs.
In conclusion, OCT has transformed glaucoma management by enabling clinicians to detect microscopic structural damage before vision is affected. The most reliable early OCT biomarkers include RNFL thinning, GCC or GCIPL thinning, BMO-MRW reduction, macular asymmetry, and early vascular density loss on OCTA. Early detection allows early treatment, early treatment preserves vision, and preserved vision ultimately maintains quality of life.